
Federal Waiver 1135 authorized temporary changes to the requirements to telehealth services for the duration of the COVID-19 Public Health Emergency and are subject to change. Given the current virus crisis, it is imperative that providers balance space availability in the reception area with the likely waiting times and accordingly schedule patients to maintain “social distance” and minimize chances of infections further spreading. Equally important, given the federal clearances and approvals, it is important for the providers to become familiar with the telehealth process and address the needs of the patients remotely. We have compiled a list of updates as well as a quick resource for providers to get the coding right and hope it is useful to the provider community who are at the front lines of fighting the pandemic!
General Information
- Federal Waiver 1135 authorized temporary changes to the requirements to telehealth services
for the duration of the COVID-19 Public Health Emergency (PHE) and are subject to change.
A. Technology: The wavier allows the use of telephones that have audio and video
capabilities.
a. Skype
b. Face Time
B. HIPAA: The OCR will waive penalties for HIPAA violations against health care providers that
serve patient in good faith through everyday communication technologies such as those
listed above during the COVID-19 PHE.
C. The waiver temporarily eliminates the requirement that the originating site must be a
physician’s office or authorized healthcare facility and allows for payment of telehealth
services in the home or any setting of care. - Place of Service is 02
- Out of Pocket applies to telehealth services but can be reduced or waived by the provider for
visits paid by federal healthcare programs. No data on what the commercial payers will allow. - Services do not have to be related to the diagnosis and or treatment of symptoms related to
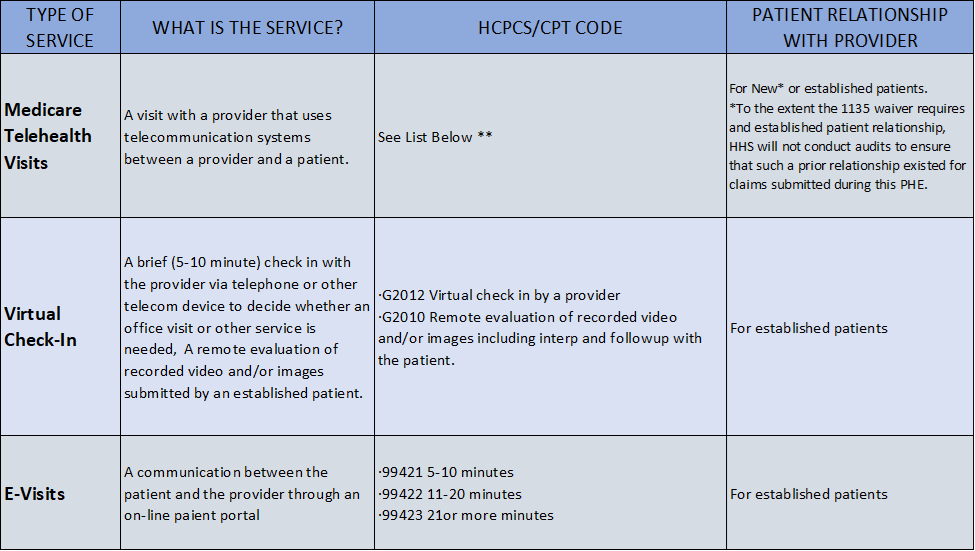
COVID-19. - There are three types of virtual services provided by physicians. These services are paid the
same rates as if the encounters were in person.
A. Virtual Check Ins- Brief communication via telephone, secure text, email, patient portal
exchange of captured video or images. These services are initiated by the patient. These
services are for established patients only.
B. E-Visits- The patient must generate the initial inquiry and verbally consent to receive virtual
check in services. These services are conducted via a patient portal. These services are for
established patients only.
C. Telehealth Visits-
a. The provider must use interactive audio and video telecommunication systems that permit real-time communication between the provider and patient.
b. The established patient requirement for these services, while recommended, will not be
validated during this PHE.
ICD10
Pneumonia:
For a pneumonia case confirmed as due to the 2019 novel coronavirus (COVID-19), assign codes
J12.89 Other viral pneumonia, and
B97.29 Other coronavirus as the cause of diseases classified elsewhere
Acute Bronchitis:
For a patient with acute bronchitis confirmed as due to COVID-19, assign codes
J20.8 Acute bronchitis due to other specified organisms, and
B97.29 Other coronavirus as the cause of diseases classified elsewhere
Bronchitis not otherwise specified (NOS) due to the COVID-19
J40 Bronchitis, not specified as acute or chronic; and
B97.29 Other coronavirus as the cause of diseases classified elsewhere
Lower Respiratory Infection
If the COVID-19 is documented as being associated with a lower respiratory infection, not otherwise specified
(NOS), or an acute respiratory infection, NOS
J22 Unspecified acute lower respiratory infection, and
B97.29 Other coronavirus as the cause of diseases classified elsewhere.
IF THE COVID-19 IS DOCUMENTED AS BEING ASSOCIATED WITH A RESPIRATORY INFECTION, NOS
J98.8 Other specified respiratory disorders
B97.29 Other coronavirus as the cause of diseases classified elsewhere
ARDS Acute respiratory distress syndrome (ARDS) may develop in with the COVID-19
J80 Acute respiratory distress syndrome, and
B97.29 Other coronavirus as the cause of diseases classified elsewhere
Exposure to COVID-19
For cases where there is a concern about a possible exposure to COVID-19, but this is ruled out after evaluation
Z03.818, Encounter for observation for suspected exposure to other biological agents ruled out.
For cases where there is an actual exposure to someone who is confirmed to have COVID-19
Z20.828, Contact with and (suspected) exposure to other viral communicable diseases
Signs and symptoms
For patients presenting with any signs/symptoms (such as fever, etc.) and where a definitive diagnosis has not
been established, assign the appropriate code(s) for each of the presenting signs and symptoms such as:
R05 Cough
R06.02 Shortness of breath
R50.9 Fever, unspecified
The information contained in this document does not guarantee payment by insurance. Contents sourced from CDC, WHO, AMA and
CMS. The above recommendations around ICD cover only a few scenarios and the choice of a particular code will be driven by underlying
diagnosis by the provider.
Please fill the below details to get copy of our article to your email ID.